These potential drug therapy problems are a good signal that the patient may benefit from pharmacy care services to clarify the medication record and work towards defining and resolving actual drug therapy problems.
An excellent starting place may be an advanced medication review or a more comprehensive assessment of a particular medical condition (as in chronic disease management). The purpose of these "initial assessments" is to clarify and assess the patients current status of care and relevant history. Afterwards, followup care is needed to follow-through on the recommendations and make sure that our interventions actually worked.
For cases where more detailed followup care is necessary, it is worthwhile to transition the patient into a defined program to give additional structure to the followup assessments. In Nova Scotia, we have the Bloom Program as a good example of this system. Patients may be enrolled in the Bloom Program if they have a drug therapy problem associated with a mental health condition. Once enrolled, they are followed by the pharmacist for ~6 months to work towards resolving problems related to their medications and improving the status of their mental health. Similar, is the Chronic Disease Management model used by the Community Pharmacy Primary Care Clinic (CPPCC) pilot project led by PANS. Except within CDM, the conditions are hypertension, diabetes, asthma, COPD and dyslipidemia instead of mental health. Really, both of these systems are pointing at a more generic "Enhanced Care" model to assist in the management of complex patient cases using defined programs.
By explicitly enrolling the patient in an enhanced care program, we are shifting our focus to a more longitudinal and clinic-based model of care.
Once the patient's condition has been stabilized, control has been achieved, or the drug therapy problems have been resolved, they can be discharged from the program and returned to usual pharmacy care for ongoing care and monitoring.
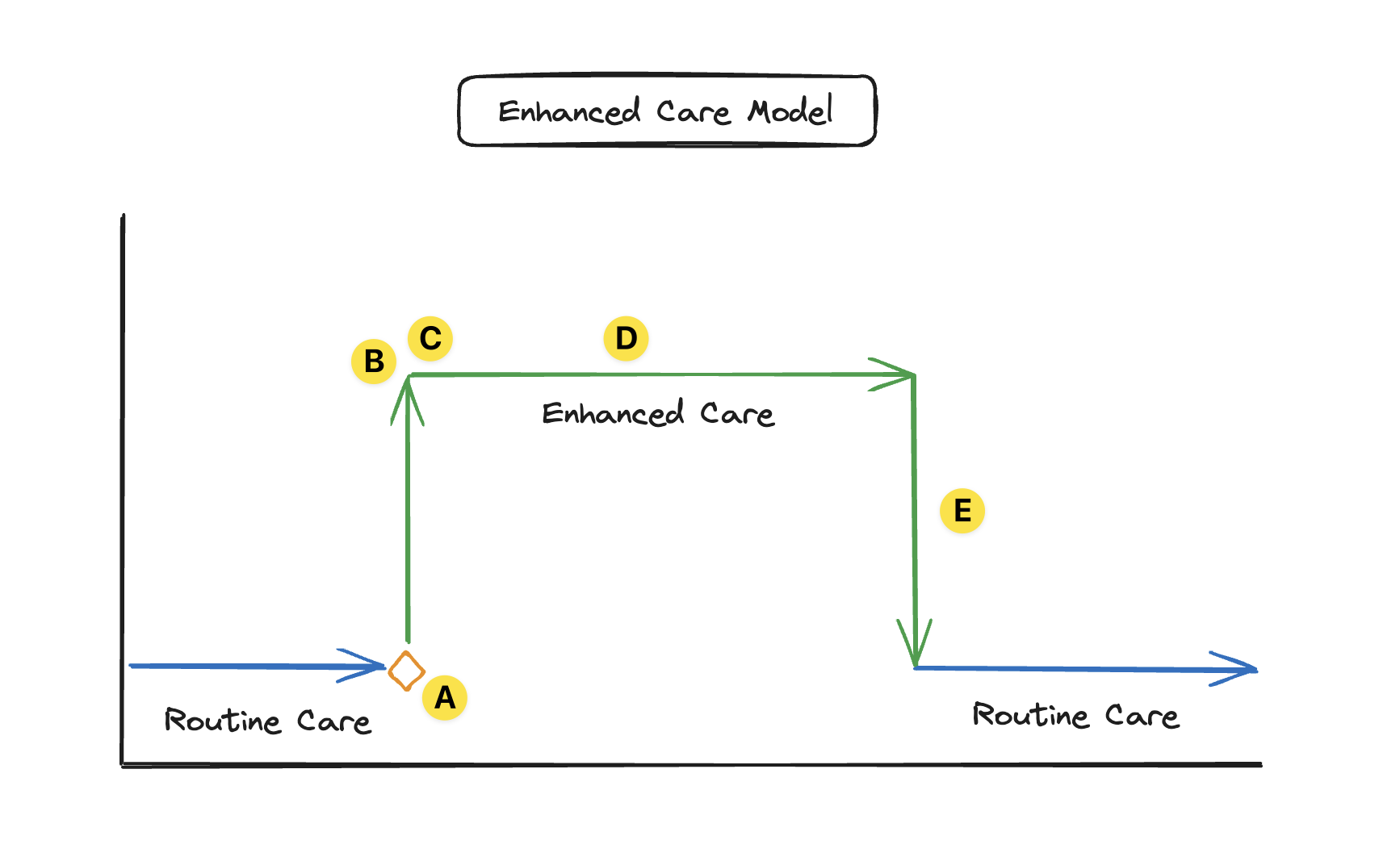 Diagram illustrating the Enhanced Care model
Diagram illustrating the Enhanced Care model
Process:
- (A) Identify pDTP(s)
- (B) Pharmacotherapy Workup (Assess, Identify DTPs)
- (C) Create care plan (interventions and monitoring plan)
- (D) Follow-up Evaluations (ongoing assessment & care planning within Enhanced Care program)
- (E) Discharge back to routine/usual care